Hip dysplasia experts may order a variety of special imaging and tests to help determine the best treatment for a patient. These are some of the most common measurements associated with evaluation of hip dysplasia. It is important to keep in mind that measurements are not always black and white, and may vary slightly between different providers (“inter-rater reliability”) and sometimes even within the same provider on multiple occasions (“intra-rater reliability”). A good hip dysplasia expert will not make a treatment plan based solely on measurements. Instead, he or she will combine information from the patient’s history, physical examination, and imaging to determine the best plan of care.
Lateral Center Edge Angle (LCEA)
This is the most commonly measured angle to determine if a person has hip dysplasia. It measures how well the acetabulum (“hip socket”) covers the head of the femur (“ball” of the hip joint).
Normal values are between 25-35 degrees
< 20-25 degrees = hip dysplasia (shallow hip socket)
> 39 degrees = over-coverage of the acetabulum and is associated with pincer impingements in femoral acetabular impingement (FAI)

Alpha Angle
The head of the femur should round. The alpha angle measures how much the shape of the femoral head differs from the normal spherical shape.
> 55 degrees is associated with CAM morphology that can be seen in femoroacetabular impingement and hip dysplasia. Notice how there is extra bone outside the circle (red arrow).

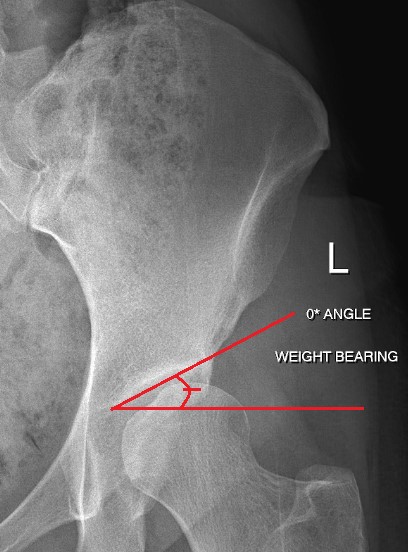
Tonnis Angle
The Tonnis angle measures the upward slope of the hip socket. A slope between 0-10 degrees is normal and allows for even loading across the joint.
>10 degrees: a steep slope may be seen with dysplasia. This increases load/stress placed across smaller parts of the joint, and can cause pain and damage to the cartilage.
< 0 degrees: a shallow slope may be seen with FAI. This can cause pain and may limit hip range of motion.
– A slope between 0-10 degrees is normal and allows for even loading across the joint.
Acetabular Index / Angle of Sharp
Hips with dysplasia have increased forces along the weight-bearing parts of the hip socket. This can cause cartilage damage and early arthritis. An increased acetabular index is seen with dysplasia and results in increased forces being loaded across a smaller surface area which causes increased pressure and stress in the joint.
> 42-45 degrees = acetabular dysplasia

Femoral Neck-Shaft Angle
This angle is formed by the line going from the center of the head of the femur down the middle of the “neck of the femur” (this is the part of the bone that connects the head (ball) of the femur to the long bone of the femur (shaft)). This measurement is used to diagnose hip conditions like hip dysplasia, FAI, Legg-Calve-Perthes disease, avascular necrosis, osteogenesis imperfecta, and fractures up near the top of the femur. This angle may be too high or too low in people with hip problems.
Normal angle =125-135 degrees
< 125 degrees = “coxa vara” (“varus”)
> 135 degrees = “coxa valga” (“valgus”)

Femoral Version
Version (or “twist”) in the femur (thigh bone) is measured by the angle between the way the head of femur is pointed and the long bone of the femur. Abnormal femoral version may be suspected during a phsyical examination, but the best imaging for measuring it is generally 3D-CT. Sometimes special MRIs can also measure femoral version.

Normal Version = 10-20 degrees forward (anteversion)
> 20 degrees = increased femoral anteversion
< 10 degrees = femoral retroversion
Increased femoral anteversion is when the top of the femur is turned forward significantly more than the long bone. People with increased femoral anteversion may walk with their toes turned in so that the head of the femur is more stable in the socket.
Femoral retroversion is when the top of the femur is turned barckwards significantly more than the long bone. People with femoral retroversion may walk with their toes turned out so that the head of the femur is more stable in the socket.

Rotation issues in the legs can be complicated and challenging to treat. Patients with abnormal rotations should be evaluated by hip preservation surgeons who specialize in patients with “version issues.” Patients with femoral anteversion or retroversion may also need to be checked for abnormal rotation in the hip socket (“acetabular anteversion” or “acetabular retroversion”) and also the tibia or “shin” bone.

References:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5193516/
https://www.sciencedirect.com/science/article/pii/S1063458413010121
https://www.sciencedirect.com/science/article/pii/S2212628717301767
https://www.hindawi.com/journals/bmri/2016/8645027/
Author: Ashley Imgrund-Flora, MS, PA-C
Illustrations by: Shian Cummings
Disclaimer: The information on the Miles4Hips website is meant for informational purposes only. While our goals are to promote understanding and knowledge of hip dysplasia and to empower patients and their families in healthcare decision making, we cannot guarantee accuracy or appropriateness of the information for your specific condition or circumstances. The information on this site is not meant to take the place of the professional judgment of your medical providers. Individuals should always seek the advice of your physician/surgeon, physical therapists, and other qualified health care provider with any questions you may have regarding a medical condition or treatment. Individuals should never disregard the advice of your medical providers or delay in seeking it because of something you have read on this website.